This moves anti-Refuge groups out of the category of harmless cranks
The people most at risk from Rocky Flats misinformation are the members of the anti-Refuge groups themselves. They are naive consumers of information and, as with most conspiracy theory groups, have a hermetically sealed set of sources of information, almost all based on discredited 40 year old sources.
For the topics below consult the more detailed documents in the Science section, where detailed citations and information is given.
The problems
Responsibility: The opposition to Refuge use is a loose affiliation of anti-nuclear groups. One group can call in support (petition signers, placard-toters, attendees at Rocky Flats Stewardship Council meetings, etc) from the others. No one takes any responsibility for nonsense strewn in their wake. There are two MDs (Sasha Stiles and Mark Johnson) loosely associated with anti-Refuge efforts, but neither has stepped up to counter medical misinformation freely passed around. Dr. Michael Ketterer, a chemist, so far has not dissociated himself from nonsense from these groups.
Expertise: Would you trust a physician or radiation oncologist who never mentions radiation dose? This is the essence of radiation epidemiology. Would he or she would never refer you for a CT scan or oppose radiotherapy for cancer? Where is their line between safe and unsafe?
The facts
Newspaper reporters and TV journalissts do not have the expertise to object to irresponsible claims. So far only Vincent Carroll of the Denver Post and Paul Karolyi’s Changing Denver podcasts on Rocky Flats have called out the activists.
Sasha Stiles’ Symposium on Rocky Flats: Impacts on the Environment and Health in late April 2022 notes that the Symposium included “critical analyses of epidemiological studies”. The talk by Mark Johnson “Nuclear Epidemiology: Who Can You Trust?” in fact contained NO epidemiology. Here’s the transcript of his talk–he punted and described the history and rising awareness of ionizing radiation, not epidemiology. Here’s the transcript (not very carefully edited or corrected). Johnson gives a handful of anecdotes about deaths at Los Alamos, the Hiroshima/Nagasaki survivors, and post-war experiments on people. Epidemiology is quantitative. The anti-nuclear activists are not.
Fearmongering
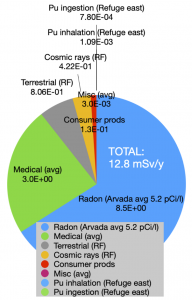
Anti-Refuge groups have no physical science or epidemiology expertise at all. As a result they ignore the issue of ionizing radiation dose, even though “The dose makes the poison”. They are happy to leave their members (and the naive public) in a state of anxiety even though radiation dose from plutonium ingested or inhaled from soil is about 4500 times smaller than the radon dose alone in a typical unmitigated basement.
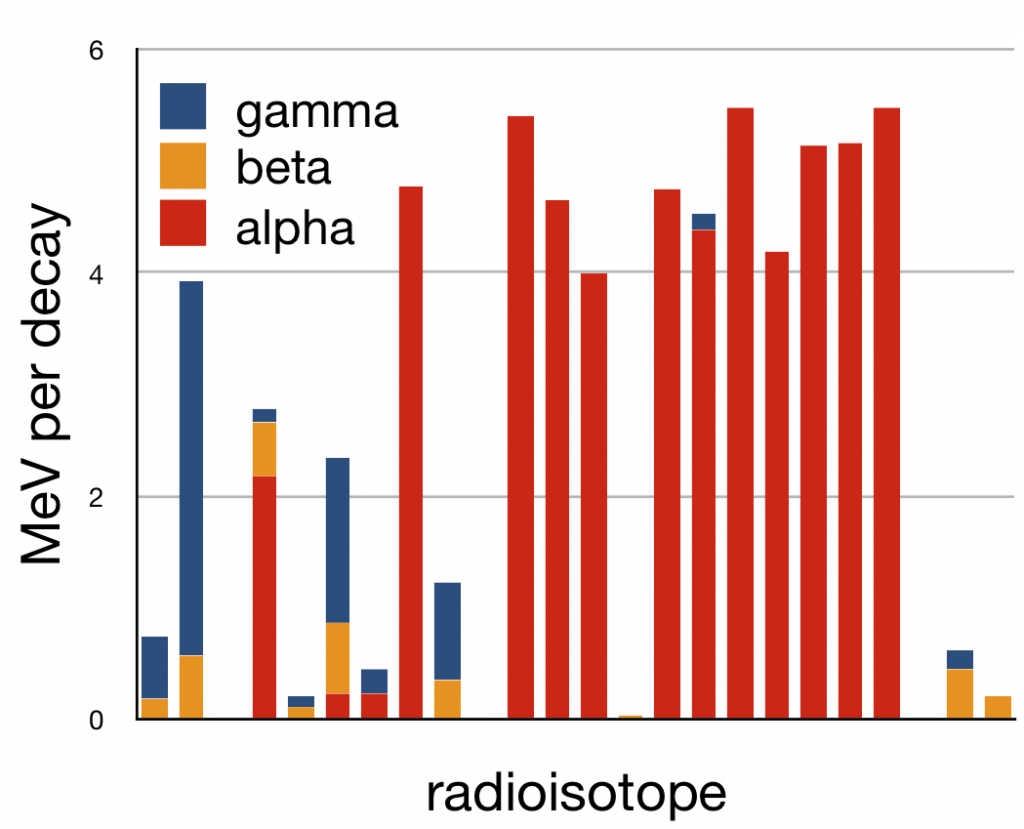
Biological toxins can be billions of times more toxic in terms of the LD50 (the dose in grams/(kg of body weight) needed to kill 50% of a population. In fact, plutonium emits many fewer gamma rays than other, natural radioisotopes in Rocky Flats soil.

Actual doses and risks
Plutonium emits almost no gamma rays, so dose comes via inhalation or swallowing. Most swallowed Pu is excreted, while inhaled PuO2 particles can become lodged in the lung. Not surprisingly, the principal health risk is thus lung cancer.
International Commission on Radiological Protection Report 150 (2021): “It is concluded that it is now possible to estimate the lifetime risk of lung cancer attributable to plutonium exposure.”
“To date, the only firm evidence for the risk of cancer in relation to plutonium exposure has been based on findings from studies of the MWC [Mayak worker cohort].”
“For the same intake, the cumulative doses to lung tissues from plutonium oxide are higher than those from plutonium nitrate, but the lifetime excess risk of lung cancer mortality per mGy varies little, with estimates between 1.4 and 1.7 per 10,000 persons, depending on the solubility (plutonium oxide or plutonium nitrate) and exposure rate (acute or chronic intake). In comparison, the lifetime baseline risk of lung cancer mortality is 631 per 10,000 persons for a Euro-American male population.'”
“For radon, there is good evidence from studies of exposure in homes to suggest that the risk of lung cancer is consistent with that estimated from studies of miners exposed at low levels…In contrast, epidemiological studies of environmental exposure to plutonium and uranium do not indicate increased risk of cancer overall. . . [italics ours]”. In other words, there is no epidemiological evidence so far of any increased risk of cancer from plutonium or uranium in the environment.
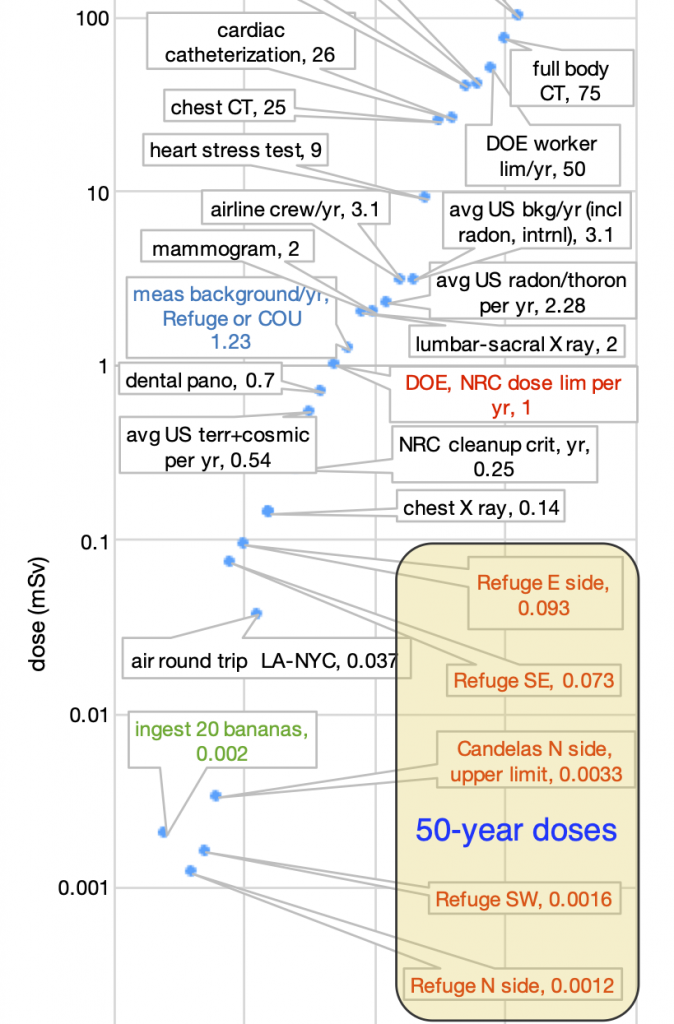
Look at the doses from Pu inhalation and ingestion below
 Radiation doses around Rocky Flats
Radiation doses around Rocky Flats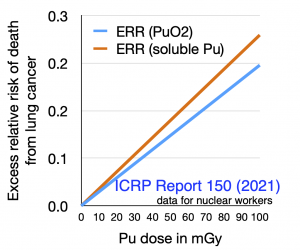 Lifetime excess risk of dying of lung cancer due to inhaling/ingesting plutonium
Lifetime excess risk of dying of lung cancer due to inhaling/ingesting plutonium
The source of all illness?
Anti-Refuge groups have no physical science or epidemiology expertise at all. As a result they ignore the issue of ionizing radiation dose, even though “The dose makes the poison”. They are happy to leave their members (and the naive public) in a state of anxiety even though radiation dose from plutonium ingested or inhaled from soil is about 4500 times smaller than the radon dose alone in a typical unmitigated basement.
Epidemiology
Repeated careful epidemiology in the 1980s (and CDPHE monitoring) has failed to show elevated cancer risks. This is as expected from the doses directly inferred from measurements. Remember that the measurement of radiation is very quantitative and reliable, the calculation of dose is somewhat less precise but is straightforward and reliable. The estimation of disease risks from very low-dose ionizing radiation is the least precise but has reached the point of predictive power for both `external’ (whole-body, gamma ray) exposure and exposure to inhaled and ingested plutonium.
‘Young breast cancer’
It is unfortunate that women with early-onset breast cancer are contacting the folks least likely to pass on useful information.
Tiffany Hansen here
“Rocky Flats Downwinders continues to be contacted by young women in the area near Rocky Flats who have been diagnosed with young breast cancer and other cancers. We need to document all health issues in the area near Rocky Flats to demand the CDPHE investigate this further. Please complete our Community Driven Health Survey here if you lived in the area of Boundaries of CO-7 on the north, I-25 on the east, I-70 on the south, and Highway 93 on the west for people who live(d), work(ed) and/or recreated in the gray area between 1952 and the present.”
While these women are being encouraged to blame Rocky Flats for their breast cancer they are failing to take actions that might actually mitigate what is an international problem.
The scientific literature in 2023
It has been known for many years that the incidence of some cancers has been increasing; colon cancer is a prominent example. Two important recent studies show that this is not a Denver area problem–it is global, and almost definitely due to lifestyle factors over which people have direct control.
Zhao J, Xu L, Sun J,et al. Global trends in incidence, death, burden and risk factors of early-onset cancer from 1990 to 2019. BMJ Oncology 2023; 2:e000049. doi:10.1136/ bmjonc-2023-000049
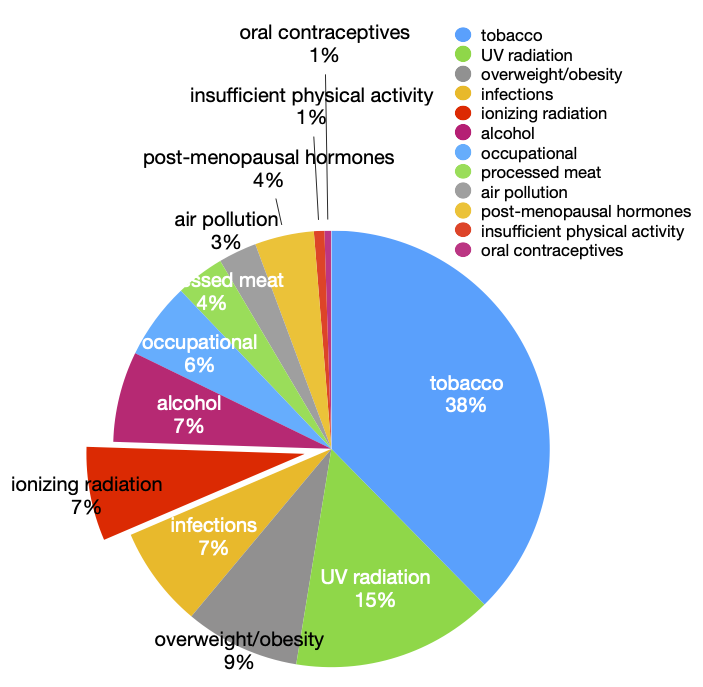
They found “Early-onset breast, tracheal, bronchus and lung, stomach and colorectal cancers showed the highest mortality and burden in 2019. Countries with a high-middle and middle Sociodemographic Index and individuals aged 40–49 years were particularly affected. Dietary risk factors (diet high in red meat, low in fruits, high in sodium and low in milk, etc), alcohol consumption and tobacco use are the main risk factors underlying early-onset cancers.”
“In 2019, the early-onset cancers with the greatest disease burden in women and men were breast cancer (348.1, 95% UI: 316.7 to 378.7 per 100k) and TBL cancer (167.6, 95% UI: 149.9 to 186.5 per 100k)”. “The highest-burden regions and cancer types were high-middle and middle SDI [socio-demographic index] regions and early-onset breast cancer, TBL cancer, CRC and stomach cancer, respectively. Dietary risk factors, alcohol use and tobacco consumption were the main risk factors for top early-onset cancers in 2019.
Koh B, Tan DJH, Ng CH, et al. Patterns in Cancer Incidence Among People Younger Than 50 Years in the US, 2010 to 2019. JAMA Netw Open. 2023;6(8):e2328171. doi:10.1001/jamanetworkopen.2023.28171
Their findings included, “In this cohort study, the incidence rates of early-onset cancer increased from 2010 to 2019. Although breast cancer had the highest number of incident cases, gastrointestinal cancers had the fastest-growing incidence rates among all early-onset cancers…. The increase in early-onset cancers is likely associated with the increasing incidence of obesity as well as changes in environmental exposures, such as smoke and gasoline, sleep patterns, physical activity, microbiota, and transient exposure to carcinogenic compounds.”
Rare cancers
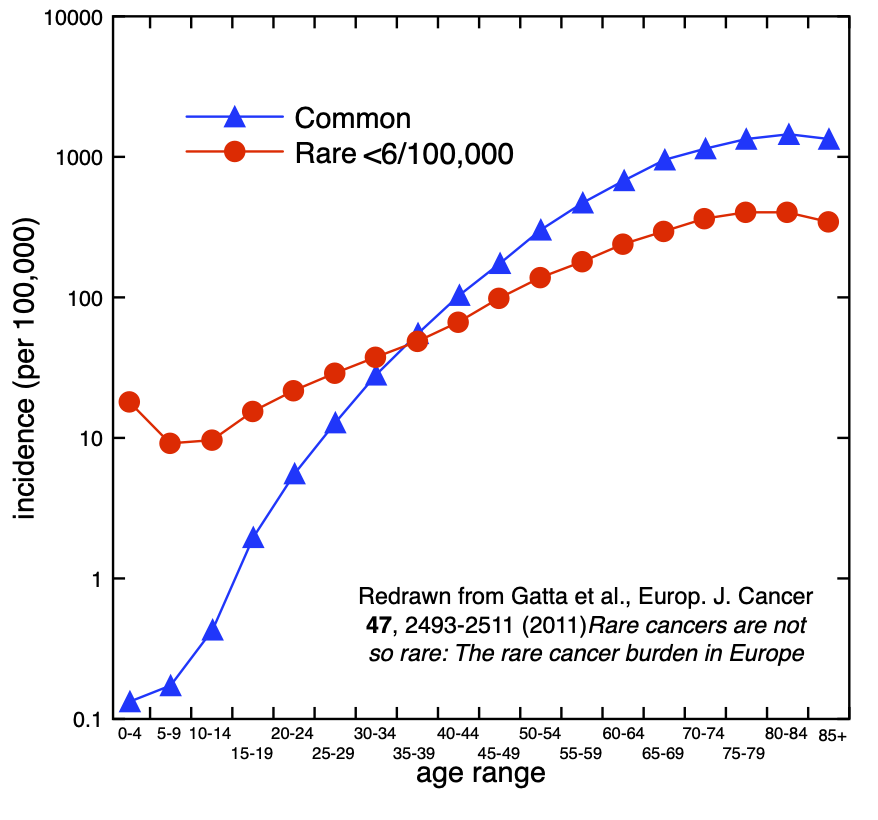
The 2016 Downwinders Health Survey was epidemiologically meaningless, but their report emphasized how frequently rare cancers occurred. Unfortunately for them, large radiation exposure causes ordinary, familiar cancers. It is also now clear that ‘rare cancers’ are not even rare.
Published epidemiology
Rare cancers are not so rare: The rare cancer burden in Europe, Gatta et al., European Journal of Cancer 47, 2493-2511 (2011)
Rare cancers are not rare in Asia as well: The rare cancer burden in East Asia, Matsuda et al, Cancer Epidemiology 67, 101702 (2020).
Increased incidence of rare cancers and varied age distributions by cancer group: A population-based cancer registry study in Hiroshima Prefecture, Japan, Cancer Epidemiology 83 102336 (2023).
This study only peripherally considered survivors of the 1945 atomic bombing but reflects epidemiological experience associated with history.
It found: “High IRs [incidence ratios] for common cancers in Japan may be responsible for the lower proportion of rare cancers in Japan compared with that in other countries…Additionally, among LSS [the Life Span Study of atomic bomb survivors] members exposed to greater than 5 mGy of radiation, the attributable fraction of radiation to solid cancer cases was 10%. Therefore, we concluded that the impact of atomic bomb radiation-associated cancer cases on cancer incidence in Hiroshima Prefecture was minimal.
I